

Denial Management Revenue Integrity
Case Studies
- All
- Alcohol Withdrawal
- Angina
- Asthma
- Bilateral Pneumonia
- Breast Cancer
- C-section
- Chest Pain
- cholecystitis
- Chronic Kidney Disease
- COPD
- Diabetes
- Diverticulitis
- Hyperemesis Gravidarum
- Inpatient
- Mastectomy
- Multiple Sclerosis
- NSTEMI
- Overdose
- Sepsis
- Short Stay
- Skilled Nursing Facility
- TKA
- Two Midnight Rule
- Type 2 Diabetes
Case Study: Medical Necessity and Reasonable Expectations
CLINICAL SUMMARY: A 73-year-old patient’s primary care doctor sent her to the Emergency Department (ED) after multiple labs taken for continuing chest pains showed abnormal results. The patient, who had been suffering chest pain for more than a week and who was taking nitroglycerin, had a stent placed in April. The patient had an extensive […]
Read More 
Case Study: Physician Advisor Secondary Review Insight on MA Case
CLINICAL SUMMARY: An 88-year-old patient with a complex cardiac history of chronic congestive heart failure and dilated cardiomyopathy arrived at the emergency department (ED) with worsening shortness of breath and intermittent dizziness. The patient’s medical history included COPD, dilated cardiomyopathy, ventricular tachycardia with implantable cardioverter-defibrillator (ICD) shocks, atrial fibrillation (for which the patient uses Eliquis®), […]
Read More 
Case Study: IPO List Proves Critical in Overturning Denied Inpatient Stay
CLINICAL SUMMARY: Doctors performed a scheduled hysteroscopy with dilation and curettage (D&C), endocervical myomectomy and MyoSure polypectomy on a 55-year-old patient who had been experiencing abnormal uterine bleeding with cervical fibroids and an endometrial polyp. The patient had a medical history which included pancreatitis due to alcoholism with a pseudocyst, deep venous thrombosis, hypertension, pleural […]
Read More 
Case Study: Denial Reversed in Short Stay Alcohol-Induced Pancreatitis Admission
CLINICAL SUMMARY: A 30-year-old patient arrived at the emergency room suffering from abdominal pain, nausea and vomiting. The patient’s symptoms had been occurring for the past six weeks and progressively worsened. The patient complained of pain in the upper abdomen that radiated to the back. The patient had a medical history of anxiety, asthma, depression, […]
Read More 
Case Study: Overnight Short-Stay Denial Reversed
CLINICAL SUMMARY: A 50-year-old patient was hospitalized overnight after arriving in the emergency room with constant left flank pain. The patient was seen in the emergency room (ER) the previous week with similar symptoms, which doctors diagnosed as a 5 mm, left proximal ureteral stone with mild hydroureteronephrosis. The patient was treated and sent home […]
Read More 
Case Study: Readmission Linking for Hospital Stays Reversed
CLINICAL SUMMARY: Recently, physicians admitted a 73-year-old patient with an extensive medical history twice within an 8-day period. The patient required inpatient level of care (LOC) for both hospitalizations. The patient was hospitalized with pneumonia during the first inpatient stay, and the second inpatient hospitalization addressed exacerbated congestive heart failure (CHF). The patient arrived for […]
Read More 
Case Study: Peer-to-Peer Review of Overlooked Medical Details Can Overturn Denials
CLINICAL SUMMARY: A 22-year-old patient, four weeks postpartum, arrived in the emergency department suffering from abdominal pain and nausea. An ultrasound revealed the common bile duct was dilated to 8 mm, and a CT scan showed gallstones. In addition to steatosis, the patient also had a positive Murphy’s sign. Lab tests performed during the patient’s […]
Read More 
Case Study: Two-Midnight Rule Helps Overturn Medicare Advantage Plan Inpatient Denial
CLINICAL SUMMARY: Two-Midnight Rule Helps Overturn Medicare Advantage Plan Inpatient Denial A 68-year-old patient with an extensive medical history arrived at the emergency room after three days of acute gastrointestinal (GI) bleeding. The patient experienced nausea and observed bright red stool blood that persisted. The patient’s medical history included atrial fibrillation treated with an […]
Read More 
Case Study: Post-Surgery Inpatient Admission Denial Overturned
CLINICAL SUMMARY: Post-Surgery Inpatient Admission Deemed Medically Unnecessary Overturned A 52-year-old patient underwent a planned ventral incisional hernia operation, performed laparoscopically using an intraperitoneal onlay mesh placement. The patient was classified as ASA Class III, defined by the American Society for Anesthesiologists (ASA) for patients with “severe systemic disease that is not incapacitating” with a […]
Read More 
Case Study: Denied One-Day Stay Overturned
CLINICAL SUMMARY: Denied One-Day Stay Overturned This case involved a patient who presented to the ER with nausea, vomiting, dry mouth, dehydration, blood sugars greater than 400 and upper abdominal pain. He was diagnosed to have DKA (diabetic ketoacidosis). This 54-year-old patient was not able to take insulin for several days leading up to this […]
Read More 
Case Study: Medical Necessity Behind Short Stay is Key
CLINICAL SUMMARY: Medical Necessity Behind Short Stay is Key This case involves a one-day inpatient denial for a 30-year-old patient treated for acute pancreatitis. With abdominal pain and nausea, the patient went to the Emergency Department where he was found to have upper abdominal pain and tenderness, a lipase of 1,447 U/L (reference range 16-77 […]
Read More 
Case Study: TKA Inpatient Status Denied Despite Being on CMS Inpatient Only List
Insurance companies are more likely to approve inpatient status for surgeries included on the CMS Inpatient Only List (IPO). Total knee replacements and total hip replacements are two common procedures on the IPO list. A Peer-to-Peer review can help reverse a denial for a inpatient stay for these types of cases. CLINICAL SUMMARY: TKA Inpatient […]
Read More 
Case Study: Awaiting Discharge to Skilled Nursing Facility
Extended hospital stays where a patient is medically ready to discharge but awaiting admission into a Skilled Nursing Facility or Acute Inpatient Rehabilitation continues to be an issue and can lead to revenue loss. AppriseMD recently overturned an inpatient denial for an 11-day hospital stay that was extended awaiting discharge. CLINICAL SUMMARY: Awaiting discharge to […]
Read More 
Case Study: Poorly Controlled Diabetes Inpatient Denial Overturned
Hospital utilization management requires constant communication between the utilization management team and physician advisors as well as continuously reassessing observation cases for possible conversion to inpatient status. Missing these opportunities leads to increased observation rates and reduced revenue. It can also lead to patients potentially requiring ongoing medical care beyond the observation period. Such patients […]
Read More 
Case Study: Total Knee Replacement Inpatient Denial Overturned
Inpatient stays for procedures commonly done on an outpatient basis can lead to denials. But appealing the denials does have promise. A recent denial for a total knee replacement that was overturned due to the patient’s high risk factors and complex medical history. CLINICAL SUMMARY: Total Knee Replacement A 67-year-old patient underwent a left total […]
Read More 
Case Study: Type 2 Diabetes and Chronic Kidney Disease
Even with concerns about days spent waiting on a transfer to a higher level of care, an insurance company medical director reversed an inpatient stay denial after a Peer-to-Peer discussion of the case. CLINICAL SUMMARY: Type 2 Diabetes and Chronic Kidney Disease A 40-year-old patient arrived in the Emergency Department complaining of worsening right upper […]
Read More 
Case Study: Asthma and High BMI
On a daily basis, hospitals must wrestle with denials for inpatient level of care for patients. An AppriseMD case review physician recently had a successful inpatient denial overturned after completing a Peer-to-Peer with an insurance company medical director regarding a case that involved a patient with asthma and a high BMI. CLINICAL SUMMARY: Asthma and […]
Read More 
Case Study: Hyperemesis Gravidarum 4-day Inpatient Stay
After overturning a four-day inpatient denial for a 13-week pregnant patient with hyperemesis gravidarum and severe pain, the insurance company medical director commented that it is very difficult to overturn these cases. Just another example of the importance of detailed follow-up Peer-to-Peer discussions, even in denied cases that seem “hopeless” to be overturned. CLINICAL SUMMARY: […]
Read More 
Case Study: Complications Following Mastectomy
A brief denial letter with limited explanation for a complicated case should not be the end of the road for a hospital claim. A recent three-day hospital stay for a patient with a history of breast cancer who underwent a left mastectomy and experienced severe postop complications was denied by the insurance company but then […]
Read More 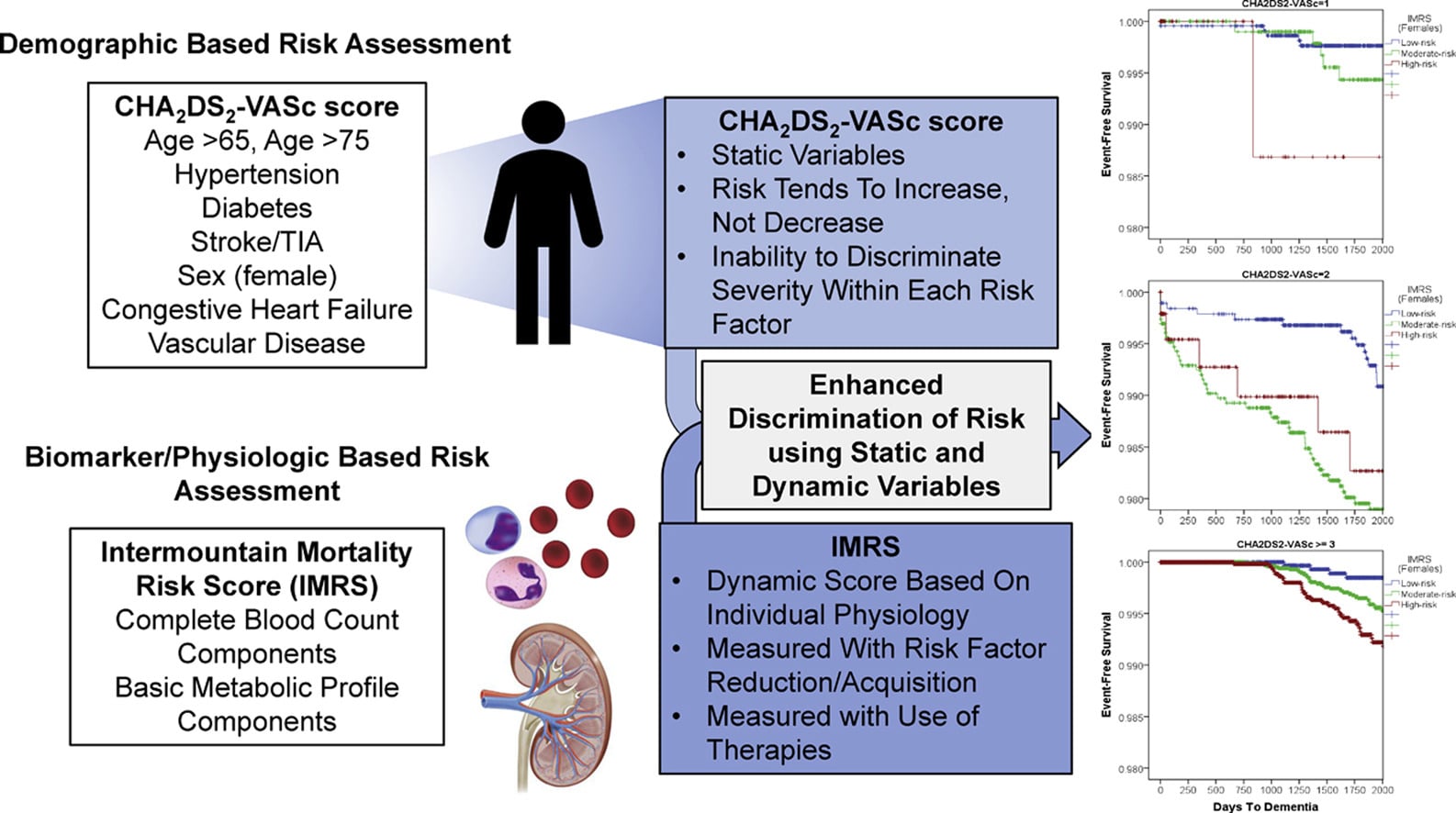
Case Study: One-day Inpatient Denial Overturned
A one-day inpatient stay for an elderly patient with a CHADS score of 4 and low EF percentage was overturned after the hospital level of care was discussed in detail during a Peer-to-Peer with the insurance company. The insurance company initially recommended an observation level of care without much explanation, but its physician overturned that […]
Read More 
Case Study: Alcohol Withdrawal and AMA Departure Can Still Qualify as Inpatient Stay
Does leaving the hospital against medical advice (AMA) equal an outpatient short stay? Not necessarily. AppriseMD reviewed one inpatient denial case involving a patient who left the hospital AMA after a two-day stay due to severe alcohol withdrawal and seizures. The AppriseMD physician reviewer was able to overturn the denial after a discussion with the […]
Read More 
Case Study: Alcohol Withdrawal Inpatient Denial Overturned Based on Care Required
Alcohol withdrawal and a positive COVID infection resulted in an inpatient hospital stay for one patient; however, the insurance company denied the short stay. A detailed peer-to-peer discussion of this case with the insurance company overturned the denial based on the acute symptoms and the medical and supportive care required. CLINICAL SUMMARY: Alcohol Withdrawal A […]
Read More 
Case Study: Multiple Sclerosis Inpatient Stay Denial Upheld
Determining level of care as a live case review can be difficult when doctors are still waiting on imaging and deciding upon treatment plans. One such live case review involved a patient with multiple sclerosis as detailed here, which AppriseMD recommended for inpatient level of care. The insurance company denied the inpatient stay. After completing […]
Read More 
Case Study: Chest Pain, Unstable Angina P2P Reveals Intricate Case
Patients admitted to the hospital with chest pain and other significant findings in the ER can still be denied for inpatient stay by insurance companies. One case involving a patient with severe stenosis of the right coronary artery and another critical lesion shows how an initial denial by the insurance company can be overturned after […]
Read More Case Study: Acute Diverticulitis Stay Denied
Healthcare insurance companies often deny inpatient hospital stays if the information provided does not show intensity of services significant enough to need inpatient care. If the patient’s care is more intense than the medical record implies a Peer-to-Peer discussion can provide more critical information to the insurance company. CLINICAL SUMMARY: Acute Diverticulitis A 69-year-old female […]
Read More 
Case Study: Post C-section Wound Infection and Asthma Exacerbation Denial Overturned
A recently denied inpatient hospital admission for asthma exacerbation and wound infection was overturned when the insurance company was made aware of additional symptoms that doctors deemed high risk and worthy of a higher level of care. Clinical information sent by the hospital to the insurance company did not show the need for the extra level […]
Read More 
Case Study: Denied Inpatient Stay Due to Suicidal Ideation and Drug Overdose Overturned
A recent case reviewed by AppriseMD showed a good example of how a case that on the surface appears inpatient appropriate can still be denied by the insurance company and overturned on peer-to-peer (P2P). Oftentimes a level-headed conversation with the insurance company will lead to the correct outcome. The case involved a drug overdose and […]
Read More 
Case Study: Sepsis Presents Challenging Denial
CLINICAL SUMMARY This case involved a 74-year-old patient who presented with chills and a temperature of 103°F. The patient had a past history of hypertension, arthritis and right total shoulder replacement in January 2021. Chest x-ray showed coarse perihilar and interstitial markings, likely viral or reactive. A CTA chest was negative for pulmonary embolism or […]
Read More 
Case Study: COPD Needing Inpatient Level of Care
CLINICAL SUMMARY This case involved an 83-year-old female patient with a known history of chronic COPD on 4L supplemental oxygen via nasal cannula, DVT, gout, multiple falls, hypertension and anxiety. She arrived in the emergency department with complaints of shortness of breath that had gotten worse over the previous 24 to 48 hours, especially on […]
Read More 
Case Study: Diabetes Patient Short Stay
CLINICAL SUMMARY This case study involves a 54-year-old female patient with a past medical history of type I diabetes, diabetic gastroparesis, nephrolithiasis, hypothyroidism, hypertension and traumatic brain injury. She arrived in the ER out of concern for diabetic ketoacidosis (DKA). The patient was hospitalized for DKA one month before this admission. She had been sick […]
Read More 
Case Study: Bilateral Pneumonia
CLINICAL SUMMARY: Bilateral Pneumonia A 23-year-old nonverbal female patient arrived in the emergency department with her parents who said she had a fever and heavy breathing since the morning. The patient’s medical history included Lennox-Gastaut Syndrome, severe mental retardation, seizure disorder, recurrent aspirations, recurrent pneumonia and vagal nerve stimulator. Her parents said she had been […]
Read More 
Case Study: Chest Pain, Non-cardiac can be Difficult to get Admission Status Correct
Chest pain is one of the most common ER diagnoses. For those patients who require hospital admission, getting the admission status correct and paid by the insurance company can be tricky. One such case involved a patient who arrived in the ER with chest pain presumed due to unstable angina (TIMI 3). The patient was […]
Read More Optimize patient care, reduce denials and maximize reimbursement through our unique approach to achieving excellence in utilization management.
Discuss your hospital’s utilization and denial management needs with our team.